When someone is diagnosed with cancer, one of the first things they hear is that chemotherapy might be part of their treatment. It’s not just a buzzword-it’s a real, powerful tool that’s been saving lives for over 70 years. But here’s the thing: chemotherapy doesn’t work in isolation. It interacts with chemotherapy drugs, over-the-counter meds, supplements, even your morning coffee in ways most patients don’t expect. And those interactions can mean the difference between recovery and a hospital trip.
How Chemotherapy Actually Works
Chemotherapy isn’t one drug. It’s a whole family of them. Some, like doxorubicin and paclitaxel, attack cancer cells by shredding their DNA. Others, like methotrexate, starve them by blocking the building blocks they need to multiply. These drugs are designed to hit fast-growing cells-which is why they work so well on cancers like leukemia and lymphoma. But they don’t know the difference between a cancer cell and a hair follicle, a gut lining, or bone marrow. That’s why side effects like hair loss, nausea, and low blood counts happen.
Doctors don’t just pick one drug and call it a day. Most regimens use combinations-like AC-T (doxorubicin and cyclophosphamide followed by paclitaxel) for breast cancer or BEP (bleomycin, vinblastine, cisplatin) for testicular cancer. Why? Because hitting cancer from multiple angles reduces the chance it will learn to resist. According to the American Cancer Society, over 70% of chemotherapy treatments today are combination therapies. This isn’t guesswork-it’s based on decades of research showing these combos kill more cancer cells than any single agent alone.
Drug Interactions You Can’t Ignore
People often don’t realize how many things they’re taking that could mess with their chemo. A common cold pill? A herbal supplement? Even grapefruit juice? All of these can change how your body handles chemotherapy.
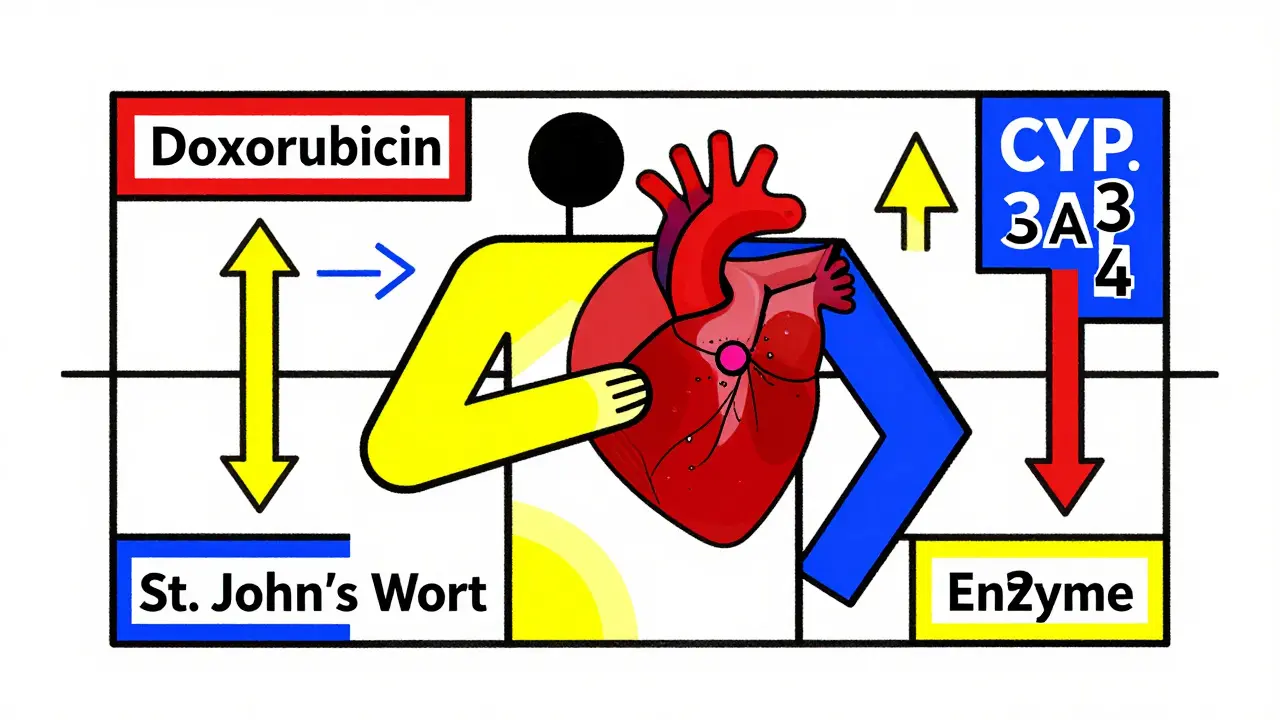
Take doxorubicin is an anthracycline chemotherapy drug used to treat breast cancer, lymphoma, and leukemia. It’s cleared by the liver through an enzyme called CYP3A4. If you’re taking St. John’s Wort-a popular herb for mood support-it boosts this enzyme. That means your body clears doxorubicin faster, so less of it reaches the cancer. Result? The treatment might not work as well.
On the flip side, some drugs slow down liver enzymes. Ketoconazole, a fungal infection treatment, can do this. If you’re on ketoconazole and get doxorubicin, the chemo builds up in your blood. That raises your risk of heart damage, which is already a known side effect of this drug. The lifetime dose limit for doxorubicin is 450-550 mg/m². Go over that, and your heart could be permanently weakened.
Even something as simple as aspirin is a nonsteroidal anti-inflammatory drug (NSAID) that can increase bleeding risk during chemotherapy can be dangerous. Many chemo drugs lower platelet counts. Add aspirin, and you’re stacking the deck for uncontrolled bleeding. The same goes for ibuprofen and naproxen. If you’re on chemo and need pain relief, acetaminophen is usually the safer pick-unless your liver is already under stress.
And don’t forget about antibiotics are medications used to treat bacterial infections, which can interfere with chemotherapy metabolism. Some, like erythromycin and clarithromycin, block the same liver enzymes that break down chemo drugs. This can cause toxic buildup. Others, like rifampin, speed up metabolism and reduce chemo effectiveness. Oncology pharmacists now routinely review every medication a patient takes-even vitamins-before chemo starts.

Why Some Patients Don’t Respond
Not everyone reacts the same way to chemotherapy. One reason? Genetics.
Take irinotecan is a chemotherapy drug used for colorectal cancer, metabolized by the UGT1A1 enzyme. About 10% of people have a genetic variant (UGT1A1*28) that makes this enzyme work poorly. If they get the standard dose, the drug builds up and causes severe, sometimes life-threatening diarrhea and low white blood cells. Since 2020, testing for this variant has been standard before starting irinotecan. If you have the variant, your dose gets cut by 30%.
Same with tamoxifen is a hormonal therapy for breast cancer that requires activation by the CYP2D6 enzyme. If you’re a poor metabolizer (about 7% of people), tamoxifen doesn’t convert to its active form. That means your cancer might keep growing. In these cases, doctors switch to aromatase inhibitors like letrozole.
These aren’t rare edge cases. Pharmacogenomic testing is now part of routine care in major cancer centers. It’s not about guessing anymore. It’s about personalizing the dose before the first treatment.
The Hidden Costs of Chemotherapy
It’s not just about the drugs. The real cost shows up in side effects that don’t show up in clinical trials.
A 2023 survey of over 1,200 patients found that 68% dealt with moderate to severe fatigue. That’s not just being tired-it’s not being able to get out of bed, skip work, or play with your kids. Another 52% still got nausea, even though they were on anti-nausea meds. And 41% developed nerve damage from taxanes like paclitaxel. That tingling in the fingers? It might not go away.
Then there’s the risk of treatment delays. About 44% of patients had their chemo postponed because their white blood cell count dropped too low (neutropenia). And here’s the kicker: Black patients were 1.7 times more likely to have delays than White patients. That’s not random-it’s tied to differences in access to supportive care, like growth factor injections or timely lab checks.
But here’s the good news: patients who got integrated palliative care-meaning pain management, emotional support, and symptom control alongside chemo-reported 35% higher quality of life and 22% fewer ER visits. That’s not a luxury. It’s part of the treatment.
What’s Changing in Chemotherapy Today
Chemotherapy isn’t disappearing. It’s evolving.
Take sacituzumab govitecan (Trodelvy) is an antibody-drug conjugate that delivers chemotherapy directly to cancer cells, reducing systemic toxicity. It’s not a traditional chemo drug. It’s a smart bomb. It attaches to a protein (TROP-2) found on cancer cells and delivers a toxic payload right to them. In triple-negative breast cancer, it cut tumor size in 35% of patients who’d tried everything else-with far fewer side effects than old-school chemo.
Another breakthrough? Using blood tests to decide how long chemo lasts. In stage II colon cancer, doctors used to give six months of treatment no matter what. Now, they check for traces of cancer DNA in the blood after surgery. If it’s gone, they stop. If it’s still there, they keep going. A 2023 study showed this cut unnecessary chemo by 32% without hurting survival rates. That’s huge. Fewer side effects. Less cost. Better quality of life.
And it’s not just about new drugs. Hospitals are getting smarter about how they give chemo. Over 90% of top cancer centers now use electronic order systems that check for drug interactions before a prescription is filled. If you’re on a drug that clashes with your chemo, the system flags it. That’s saved lives.
What You Should Do
If you or someone you love is starting chemotherapy:
- Make a full list of everything you take-prescription, OTC, supplements, herbal teas. Bring it to every appointment.
- Ask about pharmacogenomic testing. If you’re getting irinotecan or tamoxifen, insist on the test. It’s standard. If they haven’t mentioned it, ask.
- Never start a new supplement without checking with your oncology team. Even fish oil or vitamin D can interfere.
- Know your side effect red flags. Fever over 38°C? Call immediately. Diarrhea more than 4 times a day? Call. Tingling in hands or feet? Tell your nurse. Don’t wait.
- Ask for palliative care. It’s not hospice. It’s support. It helps you feel better during treatment.
Chemotherapy isn’t perfect. But it’s still one of the most effective tools we have. And when it’s used right-with the right drugs, the right dose, and the right support-it saves lives.
Can I take painkillers while on chemotherapy?
It depends. Acetaminophen (Tylenol) is usually safe. Avoid NSAIDs like ibuprofen, naproxen, or aspirin unless your doctor says yes-they can increase bleeding risk, especially if your platelets are low. Always check with your oncology team before taking anything.
Do herbal supplements interfere with chemotherapy?
Yes, many do. St. John’s Wort can make chemo less effective by speeding up liver metabolism. Milk thistle may protect the liver but can also block chemo from working. Turmeric and green tea extracts can interfere with drug breakdown. Always disclose every supplement you take-no matter how "natural" it seems.
Why do some people need lower doses of chemotherapy?
It’s often due to genetics. Some people have gene variants that affect how their body breaks down chemo drugs. For example, the UGT1A1*28 variant means irinotecan builds up to dangerous levels, so their dose is lowered. Liver or kidney problems, age, and body size also play a role. Dosing isn’t one-size-fits-all.
Is chemotherapy still used if newer treatments exist?
Absolutely. While targeted therapies and immunotherapies are growing, chemotherapy remains the backbone for many cancers. For example, in early-stage breast cancer, chemo combinations reduce recurrence by 30-40%. In fast-growing cancers like leukemia, chemo is still the fastest way to shrink tumors. Often, it’s used alongside newer drugs-not replaced.
Can chemotherapy cause permanent side effects?
Yes. Some patients develop permanent nerve damage (peripheral neuropathy) from drugs like paclitaxel. Others may have lasting heart damage from doxorubicin if they exceed lifetime dose limits. Hair texture changes and early menopause are also possible. These risks are weighed against the benefit of controlling cancer, and doctors monitor them closely.


Ivan Viktor
March 4, 2026 AT 05:13Zacharia Reda
March 5, 2026 AT 05:40Donna Zurick
March 6, 2026 AT 22:15Tobias Mösl
March 7, 2026 AT 11:00tatiana verdesoto
March 8, 2026 AT 11:48Ethan Zeeb
March 8, 2026 AT 23:36Darren Torpey
March 9, 2026 AT 03:52Mariah Carle
March 9, 2026 AT 23:10Justin Rodriguez
March 11, 2026 AT 21:02Siri Elena
March 13, 2026 AT 03:51Divya Mallick
March 14, 2026 AT 16:44Pankaj Gupta
March 15, 2026 AT 08:15Alex Brad
March 15, 2026 AT 14:22Renee Jackson
March 17, 2026 AT 09:09